Viele Aufgaben. Ein Held.

Denken Sie flexibel. Denken Sie an FlowDrya.
Synonym für Qualität & Innovation
Stronga ist ein internationales Familienunternehmen, dessen Name für Qualität bei der Entwicklung zuverlässiger, bewährter Energielösungen, Trocknungssysteme und Handhabungsprodukte steht. Unser talentiertes Team verfügt über die Erfahrung und das Know-how, um unseren Kunden qualitativ hochwertige Produkte und umfassende Geschäftslösungen zu liefern.
Unser Ziel ist es, Maschinen auf Premium-Niveau zu bauen, deren Festigkeit, Lebensdauer und Restwerte über denen anderer auf dem Markt erhältlicher Geräte liegen. Wir streben eine kontinuierliche Verbesserung unserer langlebigen Strukturen und der von uns angebotenen Dienstleistungen an und schaffen Vertrauen bei den Kunden, indem wir ihren Unternehmen einen echten Mehrwert verleihen.
HookLoada
Vielseitige, effiziente und professionelle Hakenliftanhänger
Half Pipe DumpLoada
Langlebige Halfpipe-Kipper; 20-27 Tonnen Nutzlast
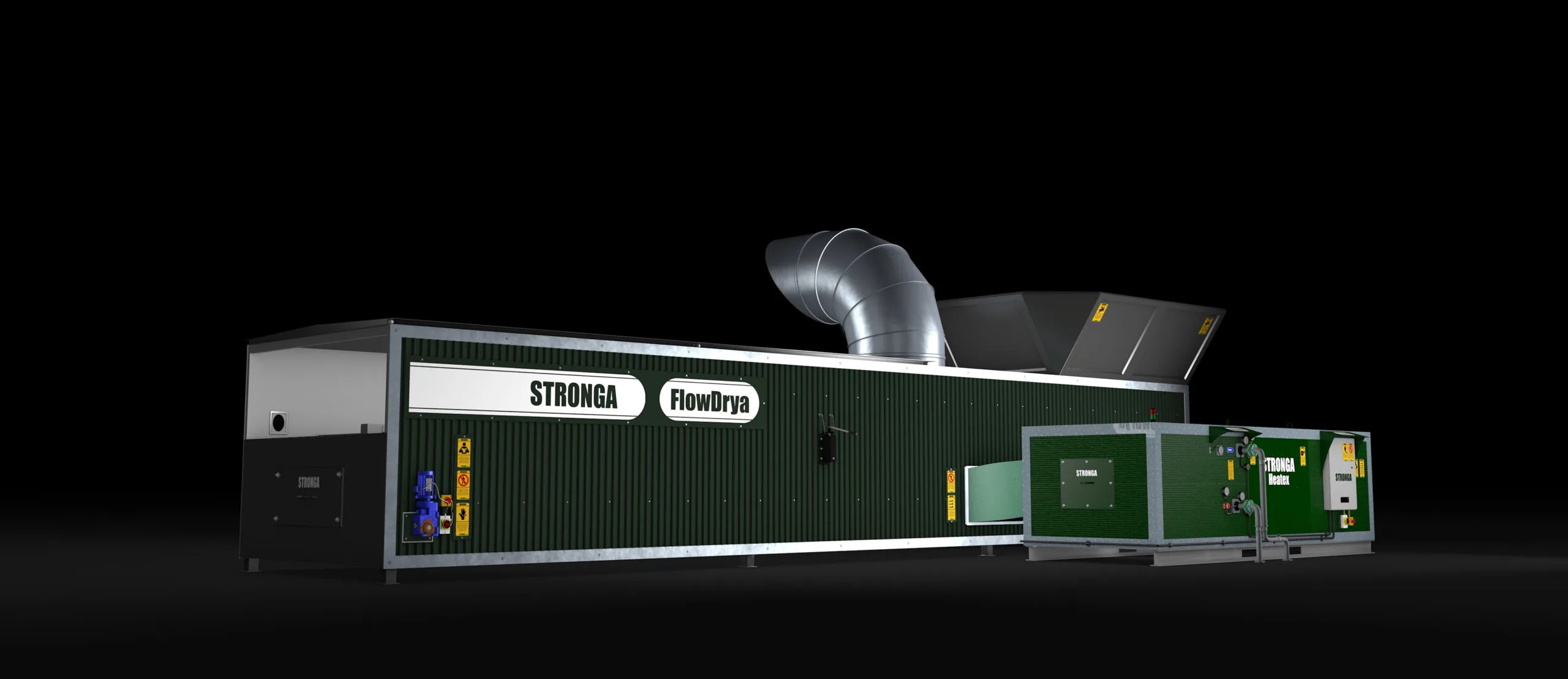
FlowDrya Green Series
Fließtrocknende feuchte Materialien, Schüttgüter und Nebenprodukte